


 Sign Out
Sign Out
Posology: Compensated liver disease: Nucleoside naïve patients: the recommended dose in adults is 0.5 mg once daily, with or without food.
Lamivudine-refractory patients (i.e. with evidence of viraemia while on lamivudine or the presence of lamivudine resistance [LVDr] mutations) (see Precautions and PHARMACOLOGY: Pharmacodynamics under Actions): the recommended dose in adults is 1 mg once daily, which must be taken on an empty stomach (more than 2 hours before and more than 2 hours after a meal) (see PHARMACOLOGY: Pharmacokinetics under Actions). In the presence of LVDr mutations, combination use of entecavir plus a second antiviral agent (which does not share cross-resistance with either lamivudine or entecavir) should be considered in preference to entecavir monotherapy (see Precautions).
Decompensated liver disease: The recommended dose for adult patients with decompensated liver disease is 1 mg once daily, which must be taken on an empty stomach (more than 2 hours before and more than 2 hours after a meal) (see PHARMACOLOGY: Pharmacokinetics under Actions). For patients with lamivudine-refractory hepatitis B, see Precautions and PHARMACOLOGY: Pharmacodynamics under Actions.
Duration of therapy: The optimal duration of treatment is unknown. Treatment discontinuation may be considered as follows: In HBeAg positive adult patients, treatment should be administered at least until 12 months after achieving HBe seroconversion (HBeAg loss and HBV DNA loss with anti-HBe detection on two consecutive serum samples at least 3-6 months apart) or until HBs seroconversion or there is loss of efficacy (see Precautions).
In HBeAg negative adult patients, treatment should be administered at least until HBs seroconversion or there is evidence of loss of efficacy. With prolonged treatment for more than 2 years, regular reassessment is recommended to confirm that continuing the selected therapy remains appropriate for the patient.
In patients with decompensated liver disease or cirrhosis, treatment cessation is not recommended.
Paediatric population: For appropriate dosing in the paediatric population, Entecavir TEVA 0.5 mg film-coated tablets are available.
The decision to treat paediatric patients should be based on careful consideration of individual patient needs and with reference to current paediatric treatment guidelines including the value of baseline histological information. The benefits of long-term virologic suppression with continued therapy must be weighed against the risk of prolonged treatment, including the emergence of resistant hepatitis B virus.
Serum ALT should be persistently elevated for at least 6 months prior to treatment of paediatric patients with compensated liver disease due to HBeAg positive chronic hepatitis B; and for at least 12 months in patients with HBeAg negative disease.
Paediatric patients with body weight of at least 32.6 kg, should be administered a daily dose of one 0.5 mg tablet with or without food.
Duration of therapy for paediatric patients: The optimal duration of treatment is unknown. In accordance with current paediatric practice guidelines, treatment discontinuation may be considered as follows: In HBeAg positive paediatric patients, treatment should be administered for at least 12 months after achieving undetectable HBV DNA and HBeAg seroconversion (HBeAg loss and anti-HBe detection on two consecutive serum samples at least 3-6 months apart) or until HBs seroconversion or there is loss of efficacy. Serum ALT and HBV DNA levels should be followed regularly after treatment discontinuation (see Precautions).
In HBeAg negative paediatric patients, treatment should be administered until HBs seroconversion or there is evidence of loss of efficacy.
Pharmacokinetics in paediatric patients with renal or hepatic impairment have not been studied.
Elderly: no dosage adjustment based on age is required. The dose should be adjusted according to the patient's renal function (see dosage recommendations in renal impairment and PHARMACOLOGY: Pharmacokinetics under Actions).
Gender and race: no dosage adjustment based on gender or race is required.
Renal impairment: the clearance of entecavir decreases with decreasing creatinine clearance (see PHARMACOLOGY: Pharmacokinetics under Actions). Dose adjustment is recommended for patients with creatinine clearance < 50 ml/min, including those on haemodialysis or continuous ambulatory peritoneal dialysis (CAPD). A reduction of the daily dose using entecavir oral solution, as detailed in the table, is recommended. As an alternative, in case the oral solution is not available, the dose can be adjusted by increasing the dosage interval, also shown in the table. The proposed dose modifications are based on extrapolation of limited data, and their safety and effectiveness have not been clinically evaluated. Therefore, virological response should be closely monitored. (See Table 8.)
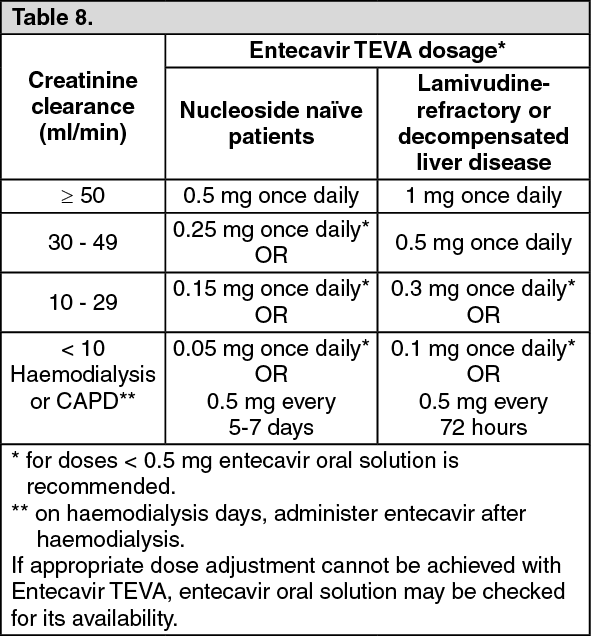 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHepatic impairment: no dose adjustment is required in patients with hepatic impairment.
Method of administration: Entecavir TEVA should be taken orally.